
PET CT Overview & Practitioner FAQs
What is a PET CT scan?
A PET CT scan simultaneously captures PET and CT images in one session for your patients. It offers comprehensive information on function, metabolism, structure, and anatomy, surpassing standalone PET or CT scans. Information gathered from PET CT imaging can aid in early disease detection, treatment monitoring, surgical planning and improve patient care.
Who can order PET CT exams?
We accept PET CT requests from all authorized licensed practitioners and physicians.
There is a common misconception that only specialists, such as cardiologists, pulmonologists, neurologists, hematologists, urologists, oncologists, etc., can order PET CT imaging and that practitioners must first refer their patients to the relevant specialist.
Does ordering a PET CT without a referral from a specialist impact patient care?
No, quite the contrary. Patients might often have to wait weeks or months before seeing a relevant specialist. Sending your patient for a PET CT scan beforehand can streamline the patient’s journey through the healthcare system.
Which patients would PET CT be appropriate for?
PET CT imaging is helpful in many applications, including cardiology, neurology, oncology, and infection/inflammation. Learn more about each application below, including case studies! If you think PET CT imaging might benefit your patient but still have questions, we suggest calling the Connect MD network!
The PCN ConnectMD Program will connect you with the appropriate dual-certified nuclear medicine physician and diagnostic radiologist from MIC to discuss your patient’s history and potential exams.
To access the PCN ConnectMD Program, call: 1-844-633-2263
What is the benefit of PET CT over conventional nuclear medicine imaging in ruling out disease?
PET differs from conventional nuclear medicine in that the images are generated on a unique camera and often combined with other radiology studies, such as computed tomography (CT).
The camera used in PET imaging can simultaneously detect two gamma-ray photons emitted from the radiotracers, whereas nuclear medicine cameras can only detect single gamma-ray photons.
The benefits of PET imaging include:
- Lower radiation dose from smaller amounts of short-lived radiotracers.
- Improved patient experience (one-day exam vs. two-day exam).
- Consistently high-quality images (sharper resolution with less background noise).
Why should I choose MIC for PET CT imaging?
MIC is the largest radiology partnership in Canada. Our 100+ radiologists play an essential role in the Edmonton area, providing diagnostic imaging services in 17 hospitals and 13 MIC clinics.
With the most sub-specialized radiologists in Alberta, MIC has the in-house expertise to be a key part of your patient’s care, from screening exams to diagnosing the most complex conditions.
MIC’s dual-certified radiologists (Diagnostic Radiology & Nuclear Medicine) are the same physicians who report PET CT studies for all indications at the University/Mazankowski and Royal Alexandra Hospitals.
Our physicians were part of the interdisciplinary team overseeing the University/Mazankowski Hospitals’ Cardiac PET Clinical Research Program in addition to multiple Health Canada-approved clinical trials bringing state-of-the-art radiotracers and PET CT imaging to Edmonton. They bring this expertise to the scanning services at MIC.
How does my patient prepare for their PET CT exam?
Exam preparation for PET CT imaging depends on the application and radiotracer.
It is imperative that your patients follow the preparation instructions closely, as improper preparation can affect the scan’s results or cause it to be rescheduled.
Our team will review the preparation with your patients when we schedule the appointment. We also have specific exam preparation instructions on our requisitions.
Can my patient travel by airplane or cross the border after their PET CT exam?
If your patients intend to travel by airplane or cross the border within 24-48 hours after their PET CT scan, they should bring their requisition indicating they have recently had a nuclear medicine imaging exam.
Most airports and border security have sensitive radiation monitors that they may trigger if they still have minute quantities of tracer in their system. Staying hydrated, drinking plenty of water, and voiding frequently after their appointment can help flush the radiotracer from their body.
How much will PET CT imaging cost my patients?
MIC uses PET CT imaging for several applications, including cardiac, oncology, and neurological imaging.
At this time, PET CT imaging in cardiac applications are covered by the Alberta Health Care Insurance Plan (AHCIP).
PET CT imaging in neurological or oncological applications are not covered by the Alberta Health Care Insurance Plan (AHCIP).
Pricing for these applications depends on the radiotracer, diagnostic enhanced CT, and personalized protocol for each patient. PET radiotracers have very short half-lives, which is beneficial for radiation exposure and imaging but makes them costly to acquire.
When we protocol an exam, the goal is to ensure that the most relevant medical imaging tests have been ordered based on clinical questions and indications. Our radiologists look at the patient’s history, region of interest, previous treatments, medical imaging, and more. More complex cases may require more imaging or contrast for CT. Our booking teams are happy to work with you and your patients to provide an accurate quote.
The cost of PET CT imaging in oncology or neurology imaging applications is as follows:
| PET CT Imaging Exam | Cost |
|---|---|
| FDG PET CT – Brain Scan | $999.00 |
| FDG PET CT – Standard Whole Body | $1,099.00 |
| FDG PET CT – Extended Whole Body | $1,199.00 |
| FDG PET CT – Head and Neck Package* | $1,499.00 |
| Dotatate PET CT | $3,299.00 |
| PSMA PET CT | $3,299.00 |
| Diagnostic Enhanced CT Scan | $499.00 |
*These prices are subject to change at any time without notice.
After our team of dual-certified radiologists protocol the exam, our booking teams will be able to provide patients with an accurate quote before committing to an appointment.
Patients are encouraged to speak to a Benefits Specialist before booking the exam to see if they qualify for extended coverage. Some extended benefits programs or health spending accounts may cover a portion or possibly the entire exam fee.
How do I book a PET CT for my patients?
Since PET CT imaging is used across a wide variety of applications, we rely on two different booking teams to help schedule appointments for your patients.
If you would like to order a PET CT for cardiac applications (myocardial perfusion imaging, viability, sarcoidosis), we ask that you:
- Please use the cardiac requisition
- Call 780.450.1500 or 1.800.355.1755
- Fax 780.450.9551
If you would like to order a PET CT for any other application (neurology, oncology – PSMA, DOTATATE, FDG), we ask that you:
- Please use the PET CT requisition
- Call 780.433.1120 or 1.888.880.1121
- Fax 780.433.7286
If you have any questions about the booking process, you can email our team at: petct@mic.ca
How long do I have to wait to see the results from my patient’s exam?
Once your patient’s appointment is complete, our radiologists will review the images and send you a detailed report, usually within 24-48 hours.
Do you have any resources about PET CT that I can share with my patients?
MIC has multiple pages about PET CT imaging and associated applications to educate patients about:
- PET vs. CT vs. PET CT
- PET CT applications (cardiology, neurology, oncology)
- How to book a PET CT appointment
- PET CT exam preparation
- What to expect during a PET CT scan
- PET CT cost (based on application)
- PET CT frequently asked questions and more!
PET CT Cardiac Applications
Cardiac PET CT imaging services at MIC include:
- Myocardial perfusion imaging (MPI)
- Myocardial viability imaging
- Cardiac sarcoidosis
General Cardiac PET CT Patient Preparation
All our PET CT cardiac applications require careful patient preparation. Generally, fasting from food and drink will be required for at least 4 – 8 hours, depending on the application selected. Our healthcare team at MIC will work with you and your patient when booking to ensure that patient preparation instructions are clearly outlined.
Cardiac PET CT Cost
All PET CT cardiac applications are covered by the Alberta Health Care Insurance Plan (AHCIP), so long as your patients have a valid Alberta Health Care card (or an out-of-province health care card, except Quebec).
Myocardial Perfusion Imaging (MPI)
Rubidium myocardial perfusion imaging (MPI) with PET CT is now available at MIC’s newly renovated Century Park clinic in South Edmonton. Your patients can expect their PET CT MPI appointment to take up to 2 hours.
Important properties of MPI PET CT:
- High accuracy – PET CT provides high sensitivity and specificity for significant obstructive coronary artery disease (CAD)
- Low radiation dose – due to the utilization of short-lived radiopharmaceuticals
- Quantification (unique to PET CT) – non-invasive myocardial blood flow measurements further improve interpretation accuracy, detection of small vessel disease and ensures an adequate stress response. PET perfusion tracers are the gold standard to non-invasively measure blood flow in the myocardium.
- Consistent, high-quality images – high spatial and contrast resolution, relatively unaffected by body shape/size
- Improved patient experience – shorter acquisition protocols achieve same-day image acquisition and study completion (versus conventional 2-day MPI SPECT protocols)
- Prognostic information – different levels of risk in scanned patient populations can be assessed
- PET CT is safe for patients with pacemakers/defibrillators, chronic renal/liver/liver disease and metallic implants (e.g. Prosthetic heart valves, sternal wires, intravascular stents).
Patient Access: MPI
PET CT MPI will be acquired at the request of the referring physician. If waitlists become long, specifically for the PET CT scanner, as per the American Society of Nuclear Cardiology (ASNC) and the Society of Nuclear Medicine & Molecular Imaging (SNMMI) position statements (Bateman et al., 2016), access will first be offered to patients who stand to benefit the most from the technology and who meet appropriate criteria for myocardial perfusion imaging and:
• Have known coronary artery disease.
• Are unable to complete a diagnostic level exercise stress imaging study (i.e. require pharmacologic stress).
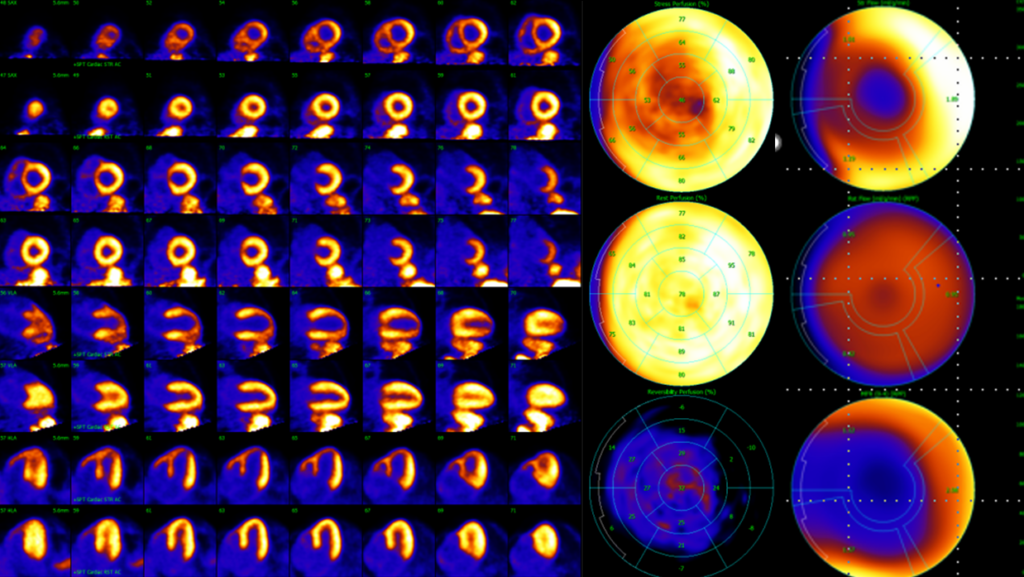
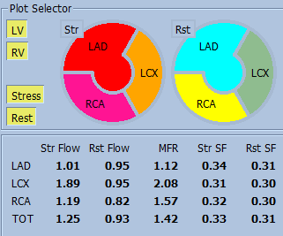
Illustration (MPI): Non-invasive quantification unique to PET CT.
Myocardial Perfusion PET CT with coronary flow quantification:
• Abnormal myocardial perfusion.
• Large area of ischemia (reversible defect) in the left anterior descending (LAD) coronary artery territory.
• Preserved left ventricular myocardial flow reserve (MFR) in other territories with a regional MFR decrease in the LAD distribution.
Myocardial Viability Imaging
Viability imaging with PET CT is now available at MIC’s newly renovated Century Park clinic in South Edmonton. Your patients can expect this appointment to take approximately 2-3 hours.
PET CT is considered the gold standard for evaluating myocardial viability by assessing metabolic activity. This application utilizes FDG to detect viable myocardium where increased glucose metabolism is a marker of cell viability. Cell viability can play an important role in treatment decisions (revascularization) and prognosis.
Patient Access: Viability
Viability assessment is only available to non-diabetic patients in the community clinic setting, like MIC.
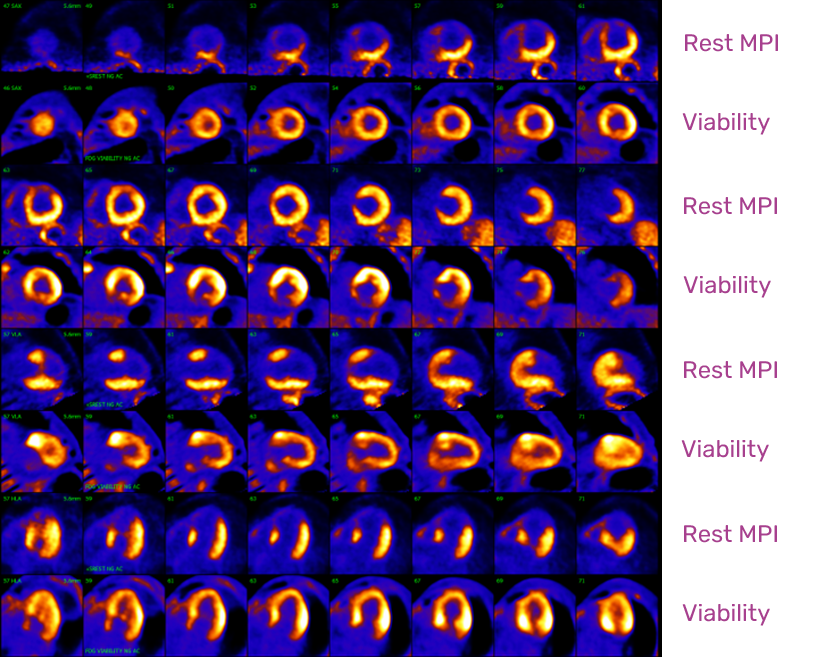
Illustration (Viability): Distinguishing hibernating myocardium that could recover from non-viable tissue. Confirming the extent of non-viable tissue.
PET Cardiac MPI with Viability Imaging: The defect on viability imaging matches the fixed myocardial perfusion defect, compatible with an inferior wall infarct. No additional viability is identified.
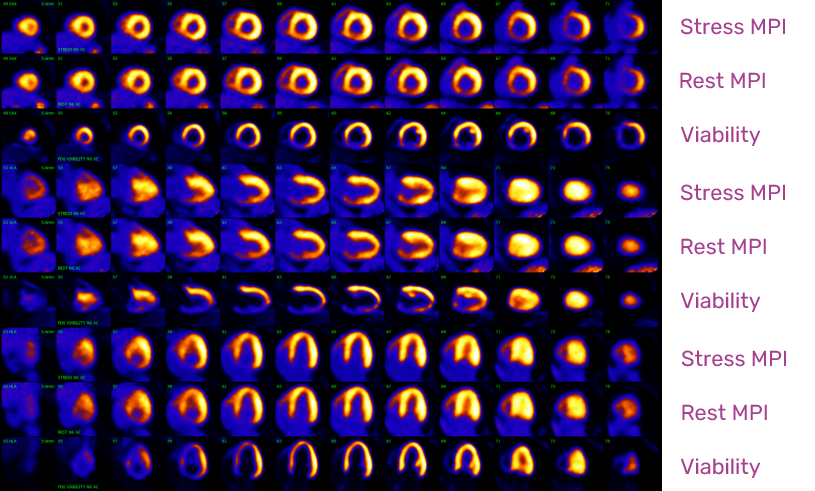
PET Cardiac MPI with Viability Imaging: Large territory of reduced perfusion to the anterior wall (LAD territory). Only mildly reduced FDG metabolism. The myocardium remains largely viable. A conventional angiogram confirms a very high-grade stenosis of LAD.
Cardiac Sarcoidosis
Cardiac sarcoidosis with PET CT is now available at MIC’s newly renovated Century Park clinic in South Edmonton. Your patients can expect their sarcoidosis PET CT appointment to take approximately 2-3 hours.
Cardiac sarcoidosis is a multi-system disease of unknown etiology characterized by the development of inflammation and noncaseating granulomas. Sarcoidosis commonly involves the pulmonary system but can involve other organ systems, including the heart.
Diagnosis
Diagnosis of cardiac sarcoidosis can be challenging when the clinical presentation is less specific. Early diagnosis can be imperative in treatment effectiveness. Imaging that can accurately identify disease, better detect disease, and extend and assess response to therapy can improve the management of cardiac sarcoidosis.
FDG PET CT for Sarcoidosis
FDG PET CT can be used to image myocardial inflammation where cellular uptake of FDG relates to inflammatory cell infiltrates. PET imaging is useful in monitoring patients who undergo immunosuppressive therapy as it has the capacity to quantify ongoing active inflammation both before and after treatment and, therefore, assess treatment response.
Assessing treatment response is particularly important as some manifestations of sarcoidosis may result from post-inflammatory scarring and persist despite successful therapy, and active sarcoidosis may also be asymptomatic.
As per the Joint SNMMI-ASNC expert consensus document (Chareonthaitawee et al., 2017), cardiac 18F-FDG PET is now included as part of the diagnostic algorithm for cardiac sarcoidosis in the Hearth Rhythm Society (HRS) criteria and is increasingly being used for detecting cardiac involvement and assessing the presence and severity of myocardial inflammation.
Cardiac Sarcoidosis General indications:
- Non-invasive diagnosis
- Therapy response
- Monitoring
- Prognosis
Clinical Scenarios in which PET CT may be useful in Suspected or Known Cardiac Sarcoidosis (CS)
- Patients with histologic evidence of extracardiac sarcoidosis and abnormal screening for CS, defined as one or more of the following:
- Abnormal electrocardiographic findings of complete left or right bundle branch block or presence of unexplained pathologic Q waves in two or more leads.
- Echocardiographic findings or regional wall motion abnormality, wall aneurysm, basal septum thinning, or LVEF < 50%Cardiac MRI findings suggestive of CS
- Unexplained palpitations or syncope
- Young patients (<60 years old) with unexplained, new onset, significant conduction system disease (such as sustained second- or third-degree atrioventricular block)
- Patients with idiopathic sustained ventricular tachycardia are defined as not fulfilling any of the following criteria:
- Typical outflow tract ventricular tachycardia
- Fascicular ventricular tachycardia
- Ventricular tachycardia secondary to other structural heart disease (coronary artery disease or any cardiomyopathy other than idiopathic)
- Patients with proven CS as adjunct to follow response treatment
Patient Access: Sarcoidosis
Patients will be assessed with a specialized dual protocol using FDG and Rubidium. Our radiologists utilize this dual protocol to compare baseline perfusion imaging and FDG PET images.
This allows for the differentiation of scar tissue from active inflammation and assessment of therapy response while excluding the possibility of hibernating/ischemic myocardium.
By also imaging the body, specificity can be further increased if positive extra-cardiac findings are identified.
Illustration (Sarcoidosis): FDG PET CT imaging of disease extent.
PET CT (A) demonstrates active sarcoidosis above AND below the diaphragm (indeterminate on conventional CT) with cardiac involvement (B) at the time of baseline evaluation. After treatment (C), the burden of active disease has significantly improved within the thorax (mediastinal nodal disease and cardiac involvement).
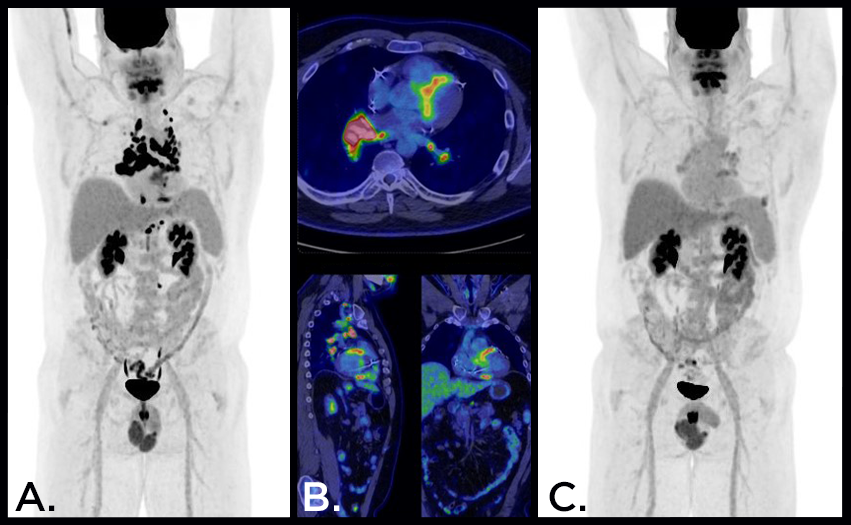
Illustration (Infection/Inflammation): Problem-solve with PET CT in challenging diagnostic cases.
PET CT can be a sensitive diagnostic technique for the evaluation of a fever of unknown origin. Patient with a fever of unknown origin and negative diagnostic CT. PET CT demonstrates large vessel vasculitis and sites of active disease.

Illustration (Infection/Inflammation): Problem-solve with PET CT in challenging diagnostic cases.
The patient was being investigated for a possible large vessel vasculitis.
Whole-body imaging with PET CT can provide a comprehensive evaluation of disease extent and can demonstrate inflammation of periarticular and articular synovial structures in overlapping polymyalgia rheumatica (PMR) or in isolated PMR.

PET CT Oncologic Applications
Oncologic PET CT imaging services at MIC utilize:
- FDG
- PSMA
- DOTATATE (SSTR)
General Oncologic PET CT Patient Preparation
Patients must prepare carefully for all oncology PET CT exams. FDG is our default tracer used in many oncology exams and has the most preparation (when compared to PSMA or DOTATATE exams). Our booking teams have been specially trained to ensure your patients are properly briefed and prepared for their exams. In general, fasting from food or drink is required for 4-6 hours.
Unique Preparation for FDG – Avoid Exercise & Stay Warm
PET imaging closely monitors changes in cellular metabolism. More active cells require more glucose to maintain their metabolism. High-energy and repetitive exercises strain muscles in the body. Similarly, thermogenic brown fat is activated to warm the body if you are too cold.
Both instances result in extra glucose going to muscle or brown fat and less available radioactive sugar for the tissue or cancer being imaged. In the end, this may result in decreased test accuracy or, in rare circumstances, a non-diagnostic test.
It is very important that patients stay warm and do not excessively stress their muscles before their appointment so we can capture high-quality images. We recommend staying warm and no intense exercise for 36 hours before the FDG PET CT appointment.
Oncologic PET CT Cost
Currently, the Alberta Health Care Insurance Plan (AHCIP) does not cover the cost of PET CT imaging used in oncologic applications (FDG, PSMA, or DOTATATE). Pricing for these applications depends on the radiotracer, area of interest, and need for a diagnostic enhanced CT accompanying the exam.
| PET CT Imaging Exam | Cost |
|---|---|
| FDG PET CT – Brain Scan | $999.00 |
| FDG PET CT – Standard Whole Body | $1,099.00 |
| FDG PET CT – Extended Whole Body | $1,199.00 |
| FDG PET CT – Head and Neck Package* | $1,499.00 |
| Dotatate PET CT | $3,299.00 |
| PSMA PET CT | $3,299.00 |
| Diagnostic Enhanced CT Scan | $499.00 |
*These prices are subject to change at any time without notice.
After our team of dual-certified radiologists protocol the exam, our booking teams will be able to provide patients with an accurate quote before committing to an appointment.
Patients are encouraged to speak to a Benefits Specialist before booking the exam to see if they qualify for extended coverage. Some extended benefits programs or health spending accounts may cover a portion or possibly the entire exam fee.
FDG PET CT (Oncology)
FDG PET CT is now available at MIC’s newly renovated Century Park clinic in South Edmonton. Your patients can expect their FDG PET CT appointment to take approximately 2-3 hours.
FDG is the most common radiotracer used in oncologic applications and is extremely valuable in optimizing treatment plans. Since FDG targets metabolically active cancer cells, it can be particularly helpful with early detection, diagnosis, tumor staging, prognosis, surveillance of recurrent disease, re-staging, radiation treatment planning, and assessing tumor response to different treatments.
The average FDG PET sensitivity and specificity across all oncology applications are estimated at 84% and 88%, respectively. The average management change across all applications is estimated to be 30% (Petersen et al., 2016).
Common Tumor Types Examined with FDG PET CT:
Breast Cancer
Breast cancer (BC) is the most frequent cancer diagnosed in women and accounts for about one in eight women diagnosed with cancer. Several treatment options (surgery, radiotherapy, chemotherapy, targeted therapy, endocrine therapy) can be used. Treatment is tailored to the biological and histological characteristics of the tumor and to the stage of the disease. Accurate staging, restaging, and response evaluation are essential for planning further optimal management.
FDG PET CT is more sensitive and specific than CT or bone scintigraphy for detecting lytic or mixed bone metastases or bone marrow involvement.
Ultrasound, mammography, axillary nodal pathologic evaluation, and breast MRI perform well in T and N staging. However, FDG PET CT can be incredibly significant for M staging. Therefore, FDG PET CT should be utilized for patients exhibiting high advanced disease risk (Stage 2B or higher) where conventional whole-body imaging will be performed for therapy planning. The detection of unsuspected malignancy alters staging, prognosis, and choice of initial therapies and management.
Learn more from a discussion/review of the literature on the role of FDG PET/CT in breast cancer.
Colorectal Cancer
Accurate initial staging is mandatory for optimal therapeutic planning. As a whole-body imaging technique, fluorodeoxyglucose (FDG) positron emission tomography (PET) and PET CT have the unique capability of providing staging for the tumor (T) stage, nodal (N) stage, and metastatic (M) stage in a single imaging session. PET CT scans prompt changes in the treatment of more than one-third of patients. PET CT can be used for the detection of tumor recurrence in the presence of CEA monitoring and also to assess resectability. Strong scientific evidence supports the use of whole-body FDG PET CT in the assessment of suspected recurrence of CRC or in the pretherapeutic staging before liver (or lung) metastasectomy. FDG PET CT should be considered a standard of care in these clinical situations.
Lung Cancer
The optimal imaging technique for lung cancer staging requires accurate characterization of the primary tumor (T), and precise assessment of local (N) and distant tumor spread (M). There is widespread consensus to use FDG PET CT for all patients with NSCLC being considered for curative-intent therapy. If patients with early-stage disease are accurately staged using FDG PET CT, inappropriate surgery can be avoided. Staging with FDG PET CT, 13.8% of patients were correctly upstaged and avoided inappropriate surgery, compared with 6.8% in the conventional imaging group. FDG PET CT imaging has a high negative predictive value for (N) thoracic lymph node evaluation, which can reduce unnecessary invasive mediastinal staging. The strength of FDG PET CT imaging, compared to conventional imaging methods for M staging in lung cancer, is to detect occult metastatic disease of adrenal glands, liver, and skeleton.
Melanoma
In the correct clinical setting, PET CT offers vertex-to-toe scans important for accurate staging and surveillance in the setting of high-risk/advanced melanoma. FDG PET CT has high overall accuracy for the detection of distant metastases and is, combined with cerebral MRI, the preferred imaging strategy for staging metastatic melanoma and also subsequently for following the patient post-treatment. FDG PET may decrease the number of additional diagnostic procedures and contribute to improved decision-making for systemic therapy options.
Myeloma
Multiple myeloma is the most common cause of primary malignancy in bones. It is a superior imaging modality to diagnose myeloma compared with conventional radiography. It provides valuable prognostic and therapy assessment information for management.
Common Oncologic Indications:
Physicians looking for a more thorough list outlining PET CT indications for oncology should visit:
INESS – Positron Emission Tomography Indications.
The resource above was written and edited by the Institut national d’excellence en santé et en services sociaux (INESSS) and is an incredibly helpful resource covering PET CT indications relating to various cancers and tumours, including but not limited to:
- Hematological cancers
- Brain tumors
- Head and neck cancers
- Lung cancer
- Digestive cancers
- Endocrine cancers
- Urological cancers
- Gynecological cancers
- Breast cancer
- Male genital cancer
- Melanoma
- Sarcomas
- Cancer of unknown primary
PET for Neuro-Oncology
FDG PET has a limited role in neuro-oncology due to high background physiologic cerebral cortical uptake. Indeed, with the exception of very aggressive malignancies like CNS lymphoma, most primary CNS neoplasms and metastatic disease has less uptake than background cerebral cortex.
However, other PET radiotracers, especially amino acid analogues like F-DOPA, FET and 11C-methionine, can successfully distinguish viable tumor from radionecrosis, both of which can have gadolinium enhancement and therefore be indistinguishable on MRI.
Finally, in selected neoplasms like meningiomas that overexpress somatostatin receptors, somatostatin receptor targeted imaging with 68Ga-DOTATATE can be used to identify residual and recurrent disease, helping to plan surgical treatment and/or radiotherapy.
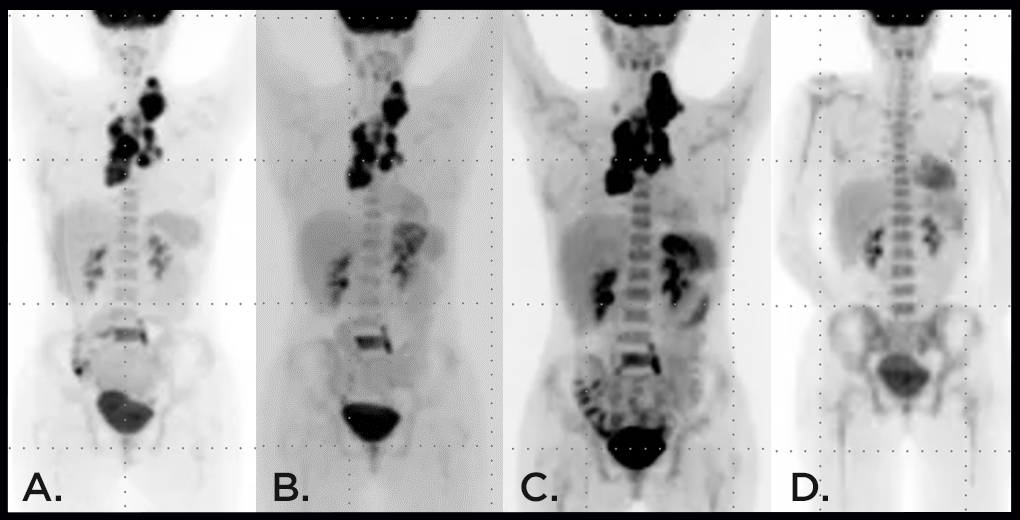
Illustration (FDG-Oncology): Optimizing treatment plans with PET CT saves time and healthcare resources.
Hodgkin’s lymphoma – Baseline initial staging scan demonstrates not only disease in nodes above the diaphragm, but previously unknown disease in the L5 vertebral body (not visible on conventional imaging and biopsy-proven) (A).
A re-assessment scan after initial therapy demonstrates stable disease (B). A re-assessment scan after continuing initial therapy demonstrates progressing disease (C).
New chemotherapy was introduced as part of a revised treatment plan. The re-assessment scan demonstrates a complete therapy response with no residual avid disease (D).
PSMA PET CT
PSMA PET CT is now available at MIC’s newly renovated Century Park clinic in South Edmonton. Your patients can expect their PSMA PET CT appointment to take approximately 2-3 hours.
PSMA PET imaging will change how prostate cancer is detected in patients and treated in Alberta and across Canada. Prostate Cancer remains the most common cancer diagnosed among Canadian men and the 2nd to 3rd most common cancer-related cause of death in men. PET CT has become an important imaging modality for the staging and re-staging of prostate cancer.
As per the joint EANM/SNMMI PSMA PET CT procedure standard (Jadvar et al., 2022), common indications for a PSMA PET CT scan include:
- Initial staging of prostate cancer (unfavourable intermediate, high or very high-risk patients)
- Localization of recurrent prostate cancer.
- Localization of prostate cancer, which is non-metastatic or metastatic by conventional imaging.
- Staging of prostate cancer prior to therapy
- Imaging metastatic castration sensitive or resistant prostate cancer.
- Monitoring treatment response or following a PSA rise after focal therapies.
- Evaluating eligibility of patients being considered for PSMA-targeted radioligand therapy.
- To guide targeted biopsies in patients with high suspicion of prostate cancer.
PSMA PET is a valid replacement for conventional imaging, providing superior accuracy to the combined CT and bone scanning in the subset of patients who are at high risk of nodal involvement.
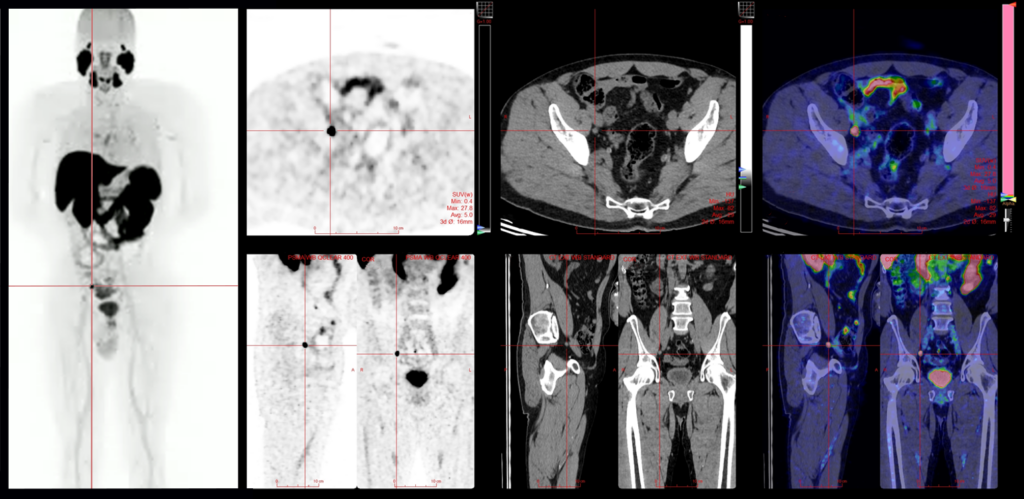
Illustration (PSMA): Optimize treatment with accurate staging.
Two patients with biopsy-proven prostate cancer and negative workup for metastatic disease (using conventional staging bone scan and CT). PSMA PET for additional workup was obtained. One only showed disease in the prostate gland, while the second showed metastases that would not have been removed at the time of surgery (with their normal bone scan for comparison).
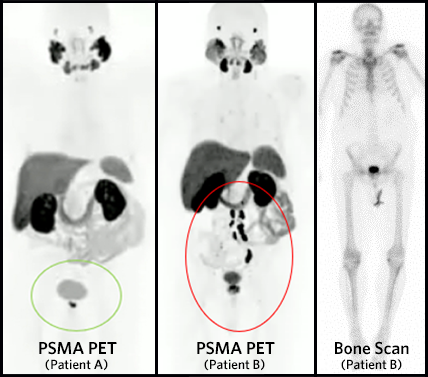
Illustration (PSMA): Identify disease otherwise not seen.
Biopsy-proven prostate carcinoma, conventional imaging normal. PSMA PET (18F-PSMA1007) shows unexpected, subsequently proven metastasis to a 5mm left perirectal lymph node.
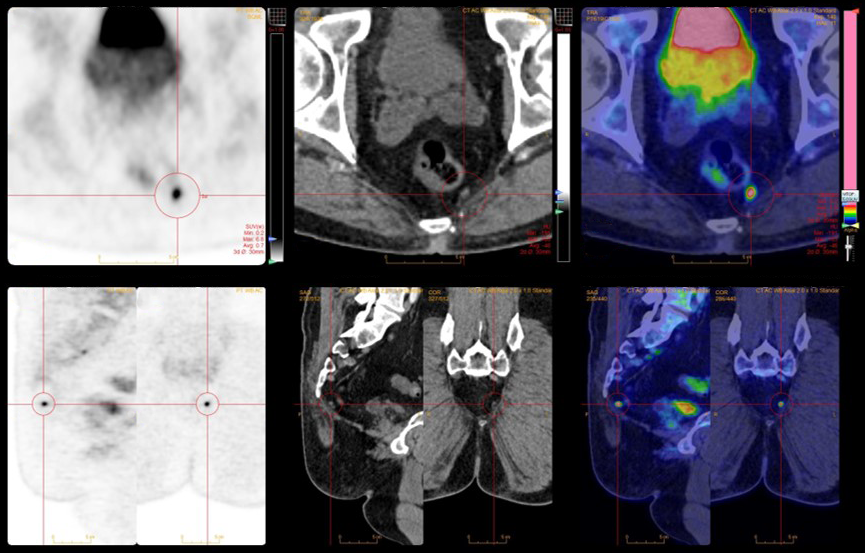
Illustration (PSMA): Use the sensitivity of PET CT to find recurrent disease.
Patient with biochemical recurrence of prostate cancer post-prostatectomy (PSA 0.89). Conventional imaging (CT and Bone scan) negative. PSMA (18F PSMA-1007) PET shows a 4mm external iliac lymph node that is consistent with a metastatic deposit (pathology-proven metastatic disease).
DOTATATE PET CT
DOTATATE (SSTR) PET CT is now available at MIC’s newly renovated Century Park clinic in South Edmonton. Your patients can expect their DOTATATE PET CT appointment to take approximately 2-3 hours.
DOTATATE PET CT is primarily used in the assessment of neuroendocrine tumors. DOTATATE may also be referred to as a Somatostatin Receptor (SSTR) PET exam. SSTR PET is the most sensitive method of detecting, staging and monitoring the treatment of well-differentiated neuroendocrine tumors (NETs)
DOTATATE PET CT is superior to traditional SPECT imaging with gamma cameras using octreotide and has essentially replaced these techniques where available. FDG PET CT and SSTR PET are complementary imaging tests depending on tumor differentiation. Well-differentiated tumors typically show high DOTATATE uptake and de-differentiated tumors are less likely to show DOTATATE uptake but will demonstrate FDG uptake.
DOTATATE (SSTR) PET General Indications:
- Diagnosis in patients with anatomic lesions that are suspicious for NET on conventional imaging.
- Detecting NETs in patients with strongly suggestive symptoms and laboratory evidence of NET but with no known primary tumor.
- Detection of NETs in patients with genetic syndromes such as multiple endocrine neoplasia type 1 or 2 and neurofibromatosis type 1.
- Staging and evaluation of the extent of disease.
- Identifying patients who are candidates for Peptide Receptor Radionuclide Therapy (PRRT) and as an adjunct to conventional imaging for response assessment after PRRT.
- Detection of and troubleshooting meningiomas
Less common DOTATATE (SSTR) PET indications:
- Medullary thyroid cancer
- Pheochromocytoma
- Medulloblastoma
- Meningioma (usually reserved for challenging cases to differentiate recurrence from post-treatment change or to assess sinus invasion)
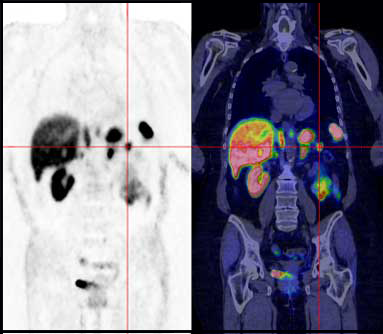
Illustration (DOTATATE): Strongly suggestive clinical symptoms & laboratory testing but negative work-up?
DOTATATE PET CT can be helpful in detecting neuroendocrine tumors – this patient presented with symptomatic hypoglycemia. Conventional imaging is unremarkable. PET CT demonstrates an avid focus in the pancreatic tail demonstrating an insulinoma, proven on subsequent resection.

PET CT Neurologic Applications
Neurologic PET CT imaging services at MIC include:
- FDG
- DOTATATE
As the vast majority of brain energy needs are supplied by glucose, the radioactive analogue 18F-fluorodeoxyglucose (FDG) can be used to detect areas of normal metabolism, decreased uptake (hypometabolism) and increased uptake (hypermetabolism).
Since normal brain FDG uptake patterns vary with age and sex, semiquantitative objective tools (statistical parametric mapping) are also used to allow for comparison of the patient’s brain FDG distribution to age and sex-matched normal controls, improving the reliability of interpretation.
Conventional Structural Imaging vs. Neurologic PET Imaging
While conventional structural imaging like CT and MRI is relied upon for the detection of vascular pathology (ischemia/infarction/hemorrhage), edema, space-occupying masses (primary CNS neoplasms, and mimickers such as infection), demyelination and some toxic/metabolic disorders, in general, structural imaging is insensitive for detecting and characterizing many neurodegenerative disorders.
These include proteinopathies causing cognitive decline (e.g., Alzheimer’s, Lewy body disease, and frontotemporal degeneration) and movement disorders (e.g., idiopathic Parkinson’s disease, atypical parkinsonian syndromes).
In contrast, these have very typical and distinct patterns of altered brain metabolism that can be identified on brain FDG PET.
FDG PET has a diagnostic accuracy that, in large systemic reviews and meta-analyses with post-mortem pathologic confirmation, matches or outperforms all other biomarker analysis methods like CSF peptide analysis.
General Neurologic PET CT Patient Preparation
Patients must prepare carefully for all neurologic PET CT exams. FDG is our default tracer used in many oncology exams and has the most preparation. Our booking teams have been specially trained to ensure your patients are properly briefed and prepared for their exams. In general, fasting from food or drink is required for 6 hours.
Neurologic PET CT Cost
Currently, the Alberta Health Care Insurance Plan (AHCIP) does not cover the cost of PET CT imaging used in neurologic applications. Pricing depends on the radiotracer and diagnostic CT accompanying the exam.
| PET CT Imaging Exam | Cost |
|---|---|
| FDG PET CT – Brain Scan | $999.00 |
| FDG PET CT – Head and Neck Package* | $1,499.00 |
| Dotatate PET CT | $3,299.00 |
| Diagnostic Enhanced CT Scan | $499.00 |
*These prices are subject to change at any time without notice.
After our team of dual-certified radiologists protocol the exam, our booking teams will be able to provide patients with an accurate quote before committing to an appointment.
Patients are encouraged to speak to a Benefits Specialist before booking the exam to see if they qualify for extended coverage. Some extended benefits programs or health spending accounts may cover a portion or possibly the entire exam fee.
FDG PET CT (Neurology)
FDG PET CT is now available at MIC’s newly renovated Century Park clinic in South Edmonton. Your patients can expect their FDG PET CT appointment to take approximately 2-3 hours.
In clinical practice, brain FDG PET can be of use in distinguishing age-related (non-progressive) cognitive decline from progressive neurodegenerative disorders, which often has great social and treatment impact.
Distinguishing between neurodegenerative disorders that can present with overlapping features (e.g., Alzheimer’s and Lewy body dementia) can help to guide appropriate therapy and avoid potential complications, such as the use of neuroleptics in Lewy body dementia.
FDG PET and Alzheimer’s
FDG PET also shows characteristic regional metabolic abnormalities in rare non-amnestic variants of Alzheimer’s like:
- Logopenic variant (a mimicker of other primary progressive aphasias).
- Posterior cortical atrophy (can have visuospatial dysfunction like Lewy body dementia).
- Frontal variant (overlapping behavioural/executive dysfunction like frontotemporal degeneration).
With the emergence of disease-modifying therapies for Alzheimer’s targeting beta-amyloid plaque, early establishment of a probable diagnosis can aid in ascertaining eligibility. While not yet routinely available in Western Canada, amyloid PET imaging can offer an alternative to more invasive lumbar puncture and CSF analysis for confirming biomarker evidence of Alzheimer’s.
FDG PET and Movement Disorders
Movement disorders are also often a clinical conundrum in establishing the underlying etiology. When atypical parkinsonian syndromes are suspected, FDG PET can show distinct metabolic abnormalities (reduced striatal uptake) from idiopathic Parkinson’s disease (preserved or increased striatal uptake).
However, the distinction of idiopathic Parkinson’s from non-neurodegenerative mimickers like essential tremor and drug-induced parkinsonism often requires imaging targeting nigrostriatal dopaminergic dysfunction, like ioflupane (DATscan) SPECT or F-DOPA PET (available only under clinical trials in Canada, including at the University of Alberta Hospital).
FDG PET and Neuroinflammatory Conditions
Neuroinflammatory conditions like encephalitis (autoimmune and paraneoplastic) and neurosarcoidosis can also be occult or subtle on MRI but frequently have severe alterations in brain metabolism on FDG PET, with both hypermetabolic (striatal, mesial temporal and frontal) and hypermetabolic (occipital).
While these patterns can have reduced specificity in the context of psychotropic medications and psychiatric spectrum illness, which can produce similar but usually less severe and less focal abnormalities, brain FDG PET can still be helpful in diagnosis and management. Moreover, in suspected paraneoplastic encephalitis, concurrent FDG PET of the body can be performed to identify occult primary neoplasms.
In medically refractory partial complex epilepsy, interictal FDG PET can be helpful in lateralization and localization of an epileptogenic focus, as these are typically asymmetrically and focally hypermetabolic.
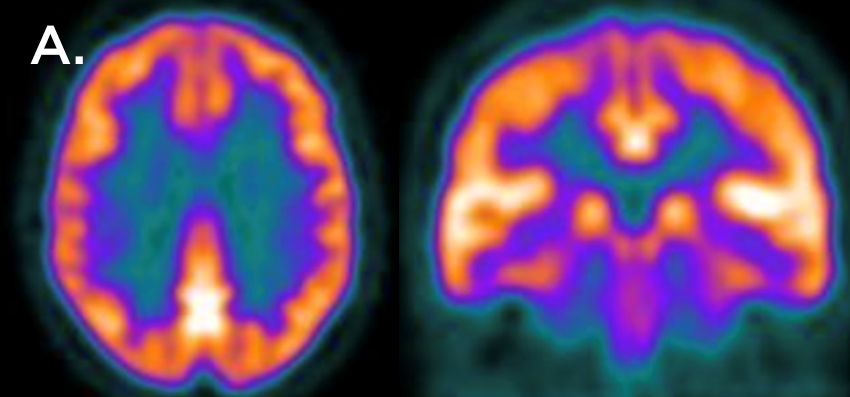
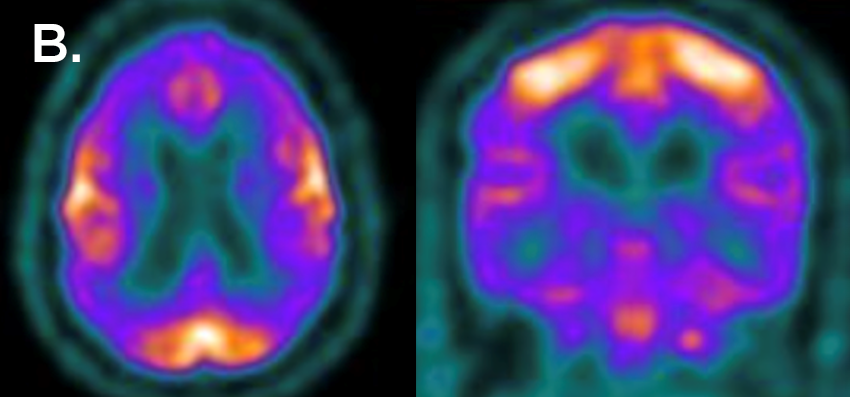
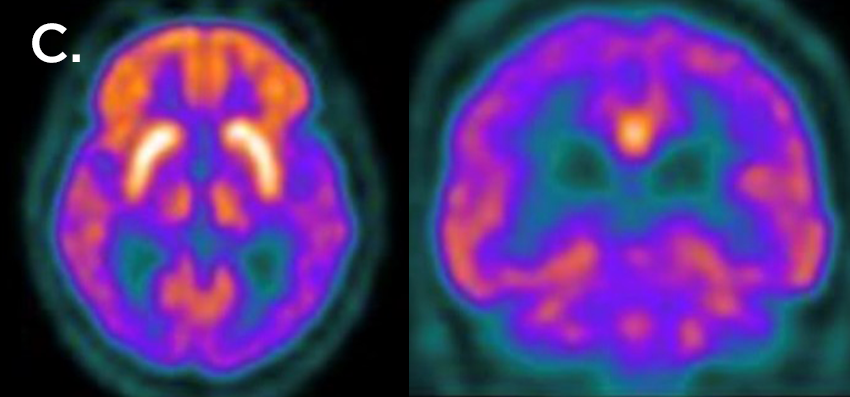
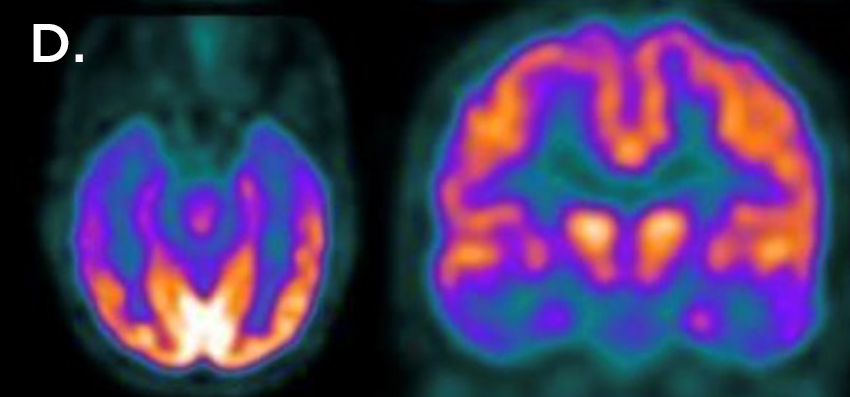
Illustration (FDG-Neurology): Detect and diagnose disease earlier.
PET of the brain demonstrates patterns of glucose metabolism that can help in differentiating Alzheimer’s disease from other causes of dementia.
The first set of images (A) show a normal brain metabolism pattern.
The second set of images (B) show a pattern characteristic of Alzheimer’s disease (even though conventional CT brain was normal).
The third set of Images (C) show a characteristic pattern of Lewy body pathology (idiopathic Parkinson’s disease or Parkinson’s disease with dementia)
The last set of images (D) show a characteristic pattern of semantic variant frontotemporal lobar degeneration (tFTLD).
American College of Radiology. (2023). ACR-ACNM-SNMMI Practice Parameter for the Performance of Gallium-68 and Copper-64 DOTATATE PET CT Imaging for Neuroendocrine Tumors. https://www.acr.org/-/media/ACR/Files/Practice-Parameters/DOTATATE_PET_CT.pdf?la=en
Bateman, T., Dilsizian, V., Beanlands, R., DePuey, G., Heller, G., Wolinsky, D. (2016). American Society of Nuclear Cardiology and Society of Nuclear Medicine and Molecular Imaging Joint Position Statement on the Clinical Indications for Myocardial Perfusion PET. Journal of Nuclear Cardiology, 23, 1227- 1231. https://doi.org/10.1007/s12350-016-0626-9
Bisschop, C., de Heer, E., Brouwers, A., Hospers, G., Jalving, M. Rational use of F-FDG PET CT in patients with advanced cutaneous melanoma: A systematic review. Critical Reviews in Oncology/Hematology; 153. https://pubmed.ncbi.nlm.nih.gov/32673997/
Boughrassa, F., Rossignol, M. (2017). Positron emission tomography: Indications. Institut national d’excellence en santé et en services sociaux (INESSS). https://www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/Oncologie/INESSS-TEPTDM_outil_interactif_EN.pdf
Brady, Z., Taylor, L., Haynes, M., Whittaker, M., Mullen, A., Clews, L., Partridge, M., Hicks, J., Trapp, V. (2008). The clinical application of PET CT: a contemporary review. Australasian Physical and Engineering Sciences in Medicine, 31(2):pp. 90-109. https://pubmed.ncbi.nlm.nih.gov/18697701/
Canadian Journal of Health Technologies. (2022). Prostate-Specific Membrane Antigen PET CT Imaging for the Staging of Prostate Cancer in Canada. https://www.cadth.ca/sites/default/files/attachments/2022-11/CM0001-PSMA-PET3.0-KH-AM-KH-KH2%20-%20with%20updates%20-%20QC-meta.pdf
Chareonthaitawee, P., Beanlands, R., Chen, W., Dorbala, S., Miller, E., Murthy, V., Birnie, D., Chen, E., Cooper, L., Tung, R., White, E., Borges-Neto, S., Di Carli, M., Gropler, R., Ruddy, T., Schindler, T., Blankstein R. (2017). Joint SNMMI–ASNC Expert Consensus Document on the Role of 18F-FDG PET CT in Cardiac Sarcoid Detection and Therapy Monitoring. Journal of Nuclear Medicine, 58 (8), 1341-1353. https://doi.org/10.2967/jnumed.117.196287
Farsad, M. (2020). FDG PET/CT in the Staging of Lung Cancer. Current Radiopharmaceuticals, 13(3):195-203. https://pubmed.ncbi.nlm.nih.gov/31868151/
Fendler, W., Eiber, M., Beheshti, M., Bomanji, J., Calais, J., Ceci, F., Cho, S., Fanti, S., Giesel, F., Goffin, K., Haberkorn, U., Jacene, H., Koo, P., Kopka, K., Krause, B., Lindenberg, L., Marcus, C., Mottaghy, F., Oprea-Lager, D., Osborne, J., Piert, M., Rowe, S., Schöder, H., Wan, S., Wester, H., Hope, T., Herrmann, K. (2023). PSMA PET CT: joint EANM procedure guideline/SNMMI procedure standard for prostate cancer imaging 2.0. European Journal of Nuclear Medicine and Molecular Imaging, 50:1466–1486. https://pubmed.ncbi.nlm.nih.gov/36604326/
Gambhir, S., Czernin, J., Schwimmer, J., Silverman, D., Coleman, R., Phelps, M. (2001). A Tabulated Summary of the FDG PET Literature. Journal of Nuclear Medicine, 42:1S–93. https://pubmed.ncbi.nlm.nih.gov/11483694/
Jadvar, H., Calais, J., Fanti, S., Feng, F., Greene, K., Gulley, J., Hofman, M., Koontz, B., Lin, D., Morris, M., Rowe, S., Royce, T., Salami, S., Baruch, B., Srinivas, S., Hope, T. (2022). Appropriate Use Criteria for Prostate-Specific Membrane Antigen PET Imaging. SNMMI procedure standards. PSMA_AUC 2022.03.15_final_BOD approved.pdf
Lonneux, M. (2008). FDG-PET and PET/CT in Colorectal Cancer. PET Clinic, 3(2):147-53. https://pubmed.ncbi.nlm.nih.gov/27156459/
Petersen, H., Holdgaard, P., Madsen, P., Knudsen, L., Gad, D., Gravergaard, A., Rohde, M., Godballe, C., Engelmann, B., Bech, K., Teilmann-Jørgensen, D., Mogensen, O., Karstoft, J., Johansen, J., Christensen, J., Johansen, A., Høilund-Carlsen, P. (2016). FDG PET/CT in cancer: comparison of actual use with literature-based recommendations. European Journal of Nuclear Medicine and Molecular Imaging, 43: 695–706. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4764641/
Ulaner, G. (2019). PET/CT for Patients with Breast Cancer: Where Is the Clinical Impact? American Journal of Roentgenol, 213(2):254-265. https://pubmed.ncbi.nlm.nih.gov/31063423/
Zhang-Yin, J. (2023). State of the Art in 2022 PET CT in Breast Cancer: A Review. Journal of Clinical Medicine, 12(3). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9917740/